
PX Leader Toolkit
Download the Respectful Handoffs Leader Guide for a team activity for building skills to "manage up" during a handoff.
ealthcare is the ultimate team sport. It requires that everyone work together to provide safe, reliable, compassionate, and quality care to patients, families, and visitors. Each of us plays an important role.
A patient’s experience begins the moment they choose or are referred to our system, which means patients interact with many individuals and teams. Each time a patient is handed off to a new team member or team, it’s an opportunity to demonstrate trust and build a feeling of safety.
What is a handoff in healthcare and why is it important?
A patient handoff is the transfer of care from one person to another. Handoffs occur frequently in health care—at the end and beginning of a shift, from front desk to medical assistant to clinician, and on the phone when being transferred.
The practice of respectful handoffs is fundamental and when used consistently, enhances the patient experience by building trust, teamwork, respect, and a greater sense of ownership for every member of the team. Among clinical teams, an effective handoff is the “key factor in fostering continuity of care and providing safe patient care.”
Consider passing patient care duties like passing a baton. That baton may be handed to us or handed off by us. At each “passing of the baton” in your work, there are communication skills that can set the stage for a more successful transfer. While there are many different ways to hand-off, using communication skills consistently is what creates impact.
Every health care setting includes handoffs
Every setting includes handoffs. For example, inpatient multidisciplinary rounding with the entire team including RNs, MDs, APCs, and others improves communication, efficiency, and effectiveness of care. In the ambulatory setting, everyone benefits from communication about wait times and setting expectations about what happens next in the visit.
Whether at the bedside, in the clinic, in the lab or radiology, as well as in the gift shop, the cafeteria, or the hall, we all play an important role in helping patients navigate their care.
Qualities of a respectful handoff
A good handoff includes the following universal qualities (you may have a structured clinical model for handoff such as SBARQ):
- Introduction: Introducing the next person who will be taking over care, including their area of focus.
- Explain action: Share a sentence or two about what the person will do to help set the stage. It’s also good for a patient or caregiver to hear something more than once. Even routine health care can feel anxious for our patients, and anxiety impacts how well people are able to absorb information.
- Manage up: Authentically sharing that you trust and respect the next person who will care for the patient builds trust for the patient. Not only does saying a few positive statements about the next person build trust for that person, it also builds trust in the entire team, unit, and the health system. You’re sharing and reinforcing that the whole team is committed to high-quality, exceptional care.
- Close: A brief wrap-up, such as thanking the patient, wishing them well, and if applicable, sharing when you’ll return, is an effective way to close the interaction.
Models for handoffs
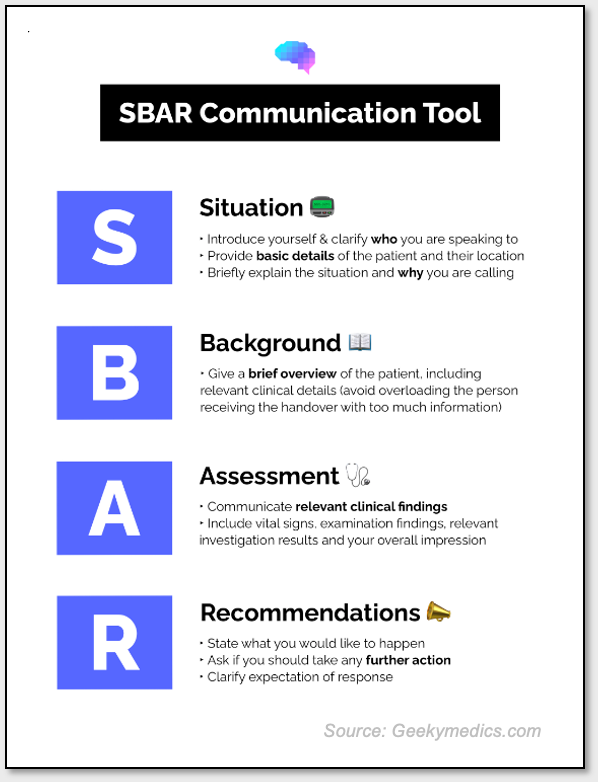 There are several models for clinical handoffs dependent on the care environment. The most popular and widely studied is SBAR (Situation, Background, Assessment, Recommendation), but there are also frameworks such as TeamSTEPPS and a “pit-stop” that may be more effective in specific environments, such as surgery. Tools like medication reconciliation and discharge planning are also forms of handoffs. Whatever model fits with your specific practice, having a structured model has been repeatedly shown to improve patient understanding of the care plan, positively influence team communication, and improve quality and safety.
There are several models for clinical handoffs dependent on the care environment. The most popular and widely studied is SBAR (Situation, Background, Assessment, Recommendation), but there are also frameworks such as TeamSTEPPS and a “pit-stop” that may be more effective in specific environments, such as surgery. Tools like medication reconciliation and discharge planning are also forms of handoffs. Whatever model fits with your specific practice, having a structured model has been repeatedly shown to improve patient understanding of the care plan, positively influence team communication, and improve quality and safety.
Best Practice Skill Building in Inpatient, Ambulatory, and ED
Inpatient Handoffs
In-hospital handoffs are common in inpatient settings—for example, hospitalized patients are often passed between doctors an average of 15 times during a single five-day hospitalization, and a typical teaching hospital may experience more than 4,000 handoffs each day. Types of handoffs include:
- Shift-to-shift handoffs (e.g., off-going RN to oncoming RN, HCA to HCA). At University of Utah Health, we have a standardized process for completing RN-to-RN bedside report.
- Nursing unit to nursing unit (e.g., Neuro Critical Care to Neuro Acute Care)
- Nursing unit to diagnostic area (e.g., Surgical Specialty to X-Ray)
- Discharge and interfacility transfer handoff (e.g., patient is discharging to long-term acute care)
- Procedures (e.g., bedside RN to PICC Team)
- Provider-to-provider handoffs (e.g., medicine to surgery)
Using the "Qualities of a respectful handoff" outlined above, this is how temporary handoff between a bedside RN to the PICC team might sound:
Introduction:
- Bedside RN and PICC team meet face-to-face
- Both parties knock and enter the patient room
- Bedside RN greets the patient and any family members
- Bedside RN introduces the PICC team: “These are my colleagues from the PICC Team. They are a specialized team that focus on venous access.”
- PICC Team colleagues introduce themselves.
Explain action:
- Bedside RN reminds patient of prior discussion: “Like we discussed this morning, your care team wanted you to have this PICC line placed so that we can access your veins and administer medications more safely. These PICC nurses are experts in this procedure.”
- PICC Team briefly explains duration of expected procedure, what to expect during, and after.
- Parties exchange any additional information using standardized protocols.
Manage up:
- Bedside RN closes their interaction with the patient: “You’re in good hands with this team. I’ll be back after the procedure to check on you.”
Close and set expectations for next steps:
- PICC Team acknowledges bedside RN: “Thanks for the introduction. We’ll check in with you after we’ve finished.”
PICC Team engages the patient in a more detailed overview of the next steps.
Ambulatory Handoffs
In the ambulatory setting, handoffs occur in two distinct ways:
- Intra-visit (between individual care team members in an individual visit progress).
- Longitudinally (between practices, services, or teams coordinating for the patient’s overall care).
In both intra-visit and longitudinal cases, the qualities of a respectful handoff apply. For example, within an outpatient clinic visit, this is how a handoff between the front desk and the MA may sound:
Introduction:
- Front Desk welcomes the patient and visitor: “Welcome in! My name is Brenda, I can help you check-in for your appointment.”
Explain action:
- Front Desk explains what is needed through the check-in process: “I’d like to ensure all of your insurance information is correct for you. Are you able to share your insurance card with me today?”
- Once checked in, Front Desk explains where to be seated and invites them to ask any questions they have: “You’re all set, let’s have you wait near this first door to be taken back. May I get you water or answer any questions?
Manage up, close and set expectations for next steps:
- Front Desk shares the approximate wait time and the name of the Medical Assistant (MA) the patient can anticipate today, along with a positive statement about the MA and Care Provider: “Lindsey and Dr. Black make a fun team to visit with. I anticipate Lindsey will be out in about 5 minutes to take you back.”
Words that reassure and set expectations can be used at multiple points during an encounter. As your patient moves from registration to rooming, from rooming and vitals to the provider, and from the provider back to MA, sharing what will happen next helps a patient understand their care and reduces anxiety.
Emergency Department Handoffs
While handoffs in the ED have been identified as a “rich source for adverse events,” they are also an opportunity for two health care providers to assess the same situation and identify a “previously unrecognized problem.”
Here is a sample framework to address the qualities of a respectful handoff in the ED:
Type of process: Because of variability in patient types and volumes in the ED, process types are often necessarily more flexible. Handoffs are often accordion-like, expanding and contracting according to patient volumes and needs.
Content: Handoffs in the ED, as in other areas, are not just a matter of communication. In addition to information, patient authority and responsibility should also be clearly transferred. This is particularly important in chaotic situations.
Structure: The nature of the participants, the number of patients involved, and the probability of the receiving party interacting with the patients are all factors that influence the structure of a handoff. These factors can combine in unique ways – for example, nurses can hand off multiple patients during lunch that the receiving nurse may not care for, nurses and providers can hand off one or multiple patients, or technicians may hand off an incoming patient with EMS.
Dynamic: Communication modes are dynamic in the ED, depending on the context of the situation. Participants may adjust their volume, detail, and style of the conversation, according to current needs.
A final note on the importance of "managing up"
Managing up (or building/lifting up) is a communication tool that positions others in a positive light. In any care setting, you can manage up by presenting your colleague’s strongest abilities to patients, referring to your colleagues by name, and making positive statements about them that demonstrate confidence and trust. You are the first source of a patient’s ability to build trust and confidence in the care team.
A team includes all key members, with patients and families at the center: consultants, nurses, APCs, PCAs, chaplains, social workers, case managers, pharmacists, phlebotomists, custodial services, etc.
Of all four qualities of a respectful handoff, “Managing up” the next person demonstrates coordination, teamwork and respect for each other’s unique expertise.
Mari Ransco
Ember Hunsaker
Kathryn Young
What do patients want? University of Utah Health’s patient experience team reveals what fifteen years of evolving qualitative analysis of hundreds of thousands of patient voices have taught us.
The patient experience team shares resources to build coordination and teamwork centered on the needs of patients, caregivers, and families.
Our words can build, or erode, trust with others. Manager of Patient Experience Operations Ember Hunsaker offers insight into how our words may be helping, or harming, those around us and how to balance the scales.