
Age Friendly Communities as Platforms for Equity, Health & Wellness

The Age-Friendly Communities Symposium brings together individuals from the Intermountain West to identify innovations and opportunities that will transform how neighborhoods, campuses, and health environments foster the independence, productivity, and wellbeing of older adults.
hen I was a family medicine resident, I was fortunate to work with a geriatrician embedded within the residency practice who inspired me to pursue a career focused on caring for older adults.
The perspective and wisdom of my older adult patients constantly inspires me. Recently, one patient proudly showed me the registration card he’d received as a participant in a polio vaccine trial. In the midst of the Covid pandemic, stories like his showcase the importance of selflessness in working towards the common good. There’s just an incredible amount of wisdom and knowledge to be gained from this group.
But because of their age, their unique experiences and conditions are sometimes dismissed by health care systems. Their needs and goals can be overlooked. Through age-friendly care practices, we can help all patients prioritize their health.
What does it mean to be an Age-Friendly Health System?
Age-friendly health systems support the unique needs of all patients, especially the aging population. Age-friendly care is an urgent need with the more than 46 million Americans aged 65 and over projected to double to more than 98 million by 2060.
University of Utah Health is proud to have received the highest possible designation for Age-Friendly Health Systems. We use the 4M’s, developed by the Institute for Healthcare Improvement, to promote high-quality evidence-based care for everyone. These four elements include:
-
What Matters Most: Understanding and aligning care to patient’s health outcome goals, including end-of-life care.
-
Medication: When necessary, prescribe age-friendly medication that reinforces the patient’s health goals.
-
Mobility: Encourage older adults to move safely daily to ensure what matters most to them.
-
Mentation: Prevent, identify, treat, and manage dementia, depression, and delirium across all aspects of care.
For age-friendly care to be effective, every interaction with an older adult–from scheduling an appointment to the clinical encounter–must consider the four M’s. But really, these four M’s are important for patients of all ages.
How to implement age-friendly care
It’s not just geriatricians that practice age-friendly care. All providers should aspire to practice age-friendly care.
Start by asking “What matters most to you?” This all-important question ultimately saves time and focuses the discussion. Understand what matters most to your patient in terms of their life and healthcare. This approach may lead to a reduction in unnecessary and unwanted care.1
Re-think medications. Once you reach 5 medications, the risk of drug interaction is virtually 100%. Try flipping the paradigm of “What drug can I add?” and consider: “Before I add drug X, can I remove drug Y?” This approach can help avoid prescribing cascades that can result from treating side effects with additional medications that result in additional side effects and drug-drug interactions.
Safely mobilize patients. Especially for inpatients, being sedentary is harmful and leads to decreased muscle mass, difficult rehabilitation, and more falls. Encourage regular mobility in a safe environment to help patients improve their quality of life.
Screen for cognitive impairment using the Mini-cog test. Take a few minutes to assess your patient’s cognition. Ask the patient to say 3 words, then draw a clock, then repeat the 3 words. Consider requesting a consultation with the Geriatrics Division’s Aging Brain Care (ABC) clinic for further evaluation if the Mini-Cog is abnormal.
Asking open-ended questions
Asking open-ended questions often feels like opening a can of worms. While you may spend a few more minutes with patients up front, that extra effort saves you (and other providers) time down the road and improves patient care.
Ask your patients to determine a goal. One of my patients wanted to attend his granddaughter’s wedding in 6 months, and another wanted to maximize their quality of life. Focus on the chronic conditions that matter most to them in the context of achieving these goals. When it comes time for treatment or surgery, ask the patient how the procedure aligns with their goals. Check in regularly about these goals, as they may shift over time.
One opportunity for health systems is to present information about what matters most to patients in a way that is accessible across different visits and practitioners. For instance, if I’ve had the “what matters most” conversation with my patients prior to surgery, I’ve saved the surgeon time because the discussion about the risks and benefits of surgery can be conducted in the context of what matters most to the patient.
This is what ageism sounds like:

Source: The Story of Reframing Aging
Words matter: Be aware of ageism
Louise Aronson, a geriatrician, writer, and professor of medicine at the University of California, San Francisco, said: "Ageism is the only -ism in which we discriminate against our future selves." If you look, you’ll see that this sentiment is unfortunately widespread in our society.
Many of us don’t realize how much ageism has infiltrated our culture, and our health care systems. It is easy to overlook how poorly age is portrayed in day-to-day interactions, the media, and in disasters like Covid-19. During the pandemic, several states had ageist provisions in resource allocation for Covid-19 treatments. Some even suggested that older adults should ‘step aside’ so the rest of the country could get on with their lives and preserve the economy.
In film and TV, older adults are often portrayed as decrepit, or a step away from a nursing home or even death.
In truth, only about 5% of US older adults require long-term care such as nursing home care. Just look at our government: most of our leaders are 65+, and many are over 80 years old. When we call older people by their first name or “honey” or “sweetie,” rather than “Mr.” or “Mrs.,” we might not recognize that this sounds disrespectful. Even the term “elderly” is considered to be disparaging; the term “older adult” should be used instead.
Ageism is discrimination, and we need to be aware of the words we use. Based on the work of the American Geriatrics Society and the Gerontological Society of America, we are reframing our language around aging.
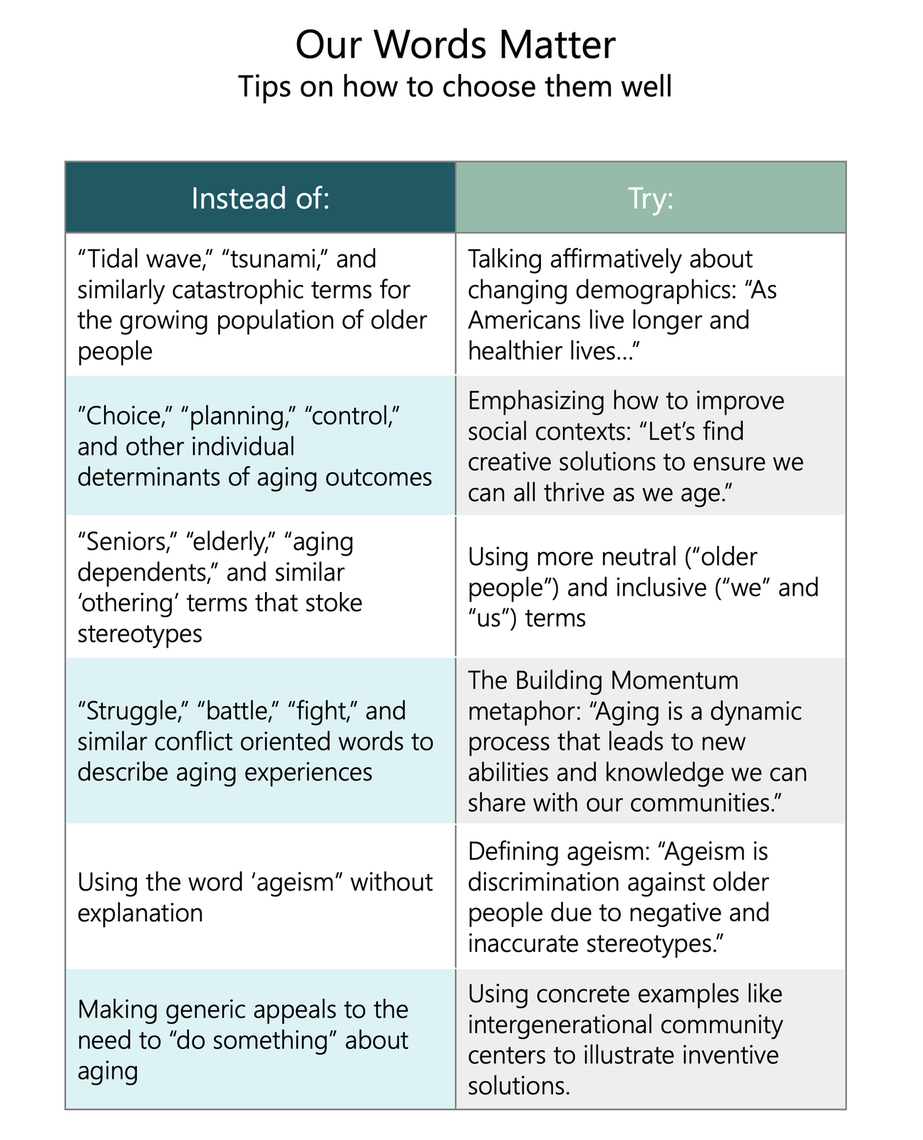
Source: The Story of Reframing Aging
Age-friendly care is for everyone
Age-friendly care applies to all patients. We should be asking everyone what matters to them, and no one should be on medications they don’t need. People should be encouraged to be mobile, and we should be monitoring their cognition. Age-friendly care benefits everybody, even if it focuses more on the older end of the age spectrum.
Reference:
- Tinetti ME et al. Association of Patient Priorities-Aligned Decision-Making With Patient Outcomes and Ambulatory Health Care Burden Among Older Adults With Multiple Chronic Conditions: A Nonrandomized Clinical Trial. JAMA Intern Med. 2019 Oct 7;179(12):1688–97
Timothy Farrell
Redwood Health Center physician Eli Moreno shares a simple exercise to cut through vaccine misinformation and empower patients to make educated decisions.
Physician Assistant and Associate Professor Joanne Rolls cares for sexual and gender minority patients and teaches new physician assistants how to comfortably approach sexual health as part of overall health. She shares practical tips to take an inclusive sexual health history.
M.ED host Kerry Whittemore interviews José E. Rodríguez, Associate Vice President for Office of Health Equity, Diversity and Inclusion, to discuss the positive changes made and efforts underway to increase diversity in the medical field.