
IMPROVEMENT TEAM: Ugolini S., MSN, RN; Dranow, L.; Sadler P.; Berry M., BSN, RN; Stehlik , J., MD; Drakos , S., MD; Nativi , J., MD; Gilbert E.M., MD; McKellar S., MD; Koliopoulou A., MD; Yin, M., MD; Davis, E., BSN, RN; Selzman , C., MD; Wever-Pinzon , O., MD.
nfection and bone marrow suppression are common complications our solid organ transplant patients experience. Even though we routinely monitor those complications, we’ve found a lot of system-wide inconsistencies related to the lab work involved. These inconsistencies can lead to repetitive blood draws, delayed results and care, increased patient charges due to multiple lab visits to collect missed or incorrect tests, and patient dissatisfaction. Our objective was to investigate whether the implementation of protocols standardizing lab order sets could result in reduced charges for solid organ transplant recipients.
Spotting hidden variations in labs
We conducted a series of PDSA cycles and identified variations in the types of labs ordered and by different providers across the hospital. Then we identified two labs to focus our energy on:
1. Complete Blood Count (CBC) vs. CBC with differential:
Because the CBC w/ diff test breaks white blood cells out into five different categories, providers often don’t order it because they assumed it’s more expensive. It sounds counterintuitive, but a CBC actually costs more than a CBC w/ diff.
2. Cytomegalovirus (CMV) vs. CMV-Polymerase Chain Reaction (PCR):
The CMV test is qualitative, measuring the presence or absence of CMV, while CMV-PCR is quantitative, measuring the amount of virus present. These labs were often erroneously interchanged and ordered incorrectly, even though CMV-PCR has a lower patient charge than CMV.
Collaborating with a cross-functional team
We pulled and reviewed a sample of heart transplant orders from a cohort of 500 patients who received liver, heart, and kidney transplants in FY16. Then, we compared that data set with existing clinical practice guidelines for all organ transplant groups to identify and ensure appropriate clinical care. On the facilities side, we contacted the hospital operations billing department and asked them to run a report of the charges billed to the patient for each of those labs.
With guidelines and charges in hand, we then presented the information to the physician groups. We found that ordering tests with lower charges did not compromise patient care. Those tests provided the exact data that physicians needed–they were very receptive to the change. Currently, when providers order tests, they don’t know the associated charges, which leaves them blind to a patient’s financial outcomes. With the data in hand, physicians could start to make informed decisions in their practice that had a direct impact on quality and patient charges.
Implementing new protocols
Finding these inconsistencies and sharing them with the team, we quickly realized that we could translate the findings to other organ groups who order these labs. With provider input, we identified tests with lower charges that were still clinically safe and created new protocols for ordering them.
We minimized order variability by creating a new standardized Smart Set and uploading it into Epic, where only the clinically appropriate lab with lower charges shows up. That served as a forcing function, actually preventing ordering errors that typically occur from manual entry of labs.
To further avoid erroneous or missing tests, we educated staff and patients about our changes and then assessed and monitored the outcomes. We met quarterly as a group and compared the proportions of incorrect tests and associated patient charges between the pre- and post-protocol era labs.
The results by the numbers
Standardizing post-transplant laboratory testing in solid organ transplant recipients resulted in a reduced number of inappropriate tests and lower associated patient charges. These changes could be translatable across other disciplines and implemented in other facets of patient care.
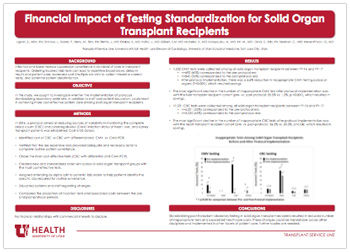
Of 1,532 CMV tests collected among all solid organ transplant recipients between FY16-FY17:
- 692 (45%) ordered pre-implementation
- 840 (55%) ordered post-implementation
After implementation, there was a 6.6% reduction in inappropriate CMV testing across all organs (P<0.001), which resulted in savings.
- The most significant decline in the number of inappropriate CMV test after protocol implementation was with the liver transplant recipient cohort (pre- vs. post-protocol: 33.5% vs. 1.2%, p <0.001), which resulted in savings.
Of 11,231 CBC tests collected among all solid organ transplant recipients between FY16- FY17
- 6,201 (55%) ordered pre-implementation
- 5,030 (45%) ordered post-implementation
- The most significant decline in the number of inappropriate CBC tests after protocol implementation was with the heart transplant recipient cohort (pre- vs. post-protocol: 26.2% vs. 20.3%, p=0.04), which resulted in savings.
Improvement that can spread
Though savings are modest in the study sample (n=500), if we take into consideration the thousands of patients these labs are ordered for regularly, you can begin to understand the potential impact if implemented broadly.
The broader result is that we actually look more intently at what tests we order. Physicians were eager to understand the financial impact to the patient of labs; that allowed them to incorporate appropriate decision-making into their test ordering process. And that increases value for patients. They no longer have to come back and be redrawn for the wrong test. Sometimes we don’t acknowledge the patient impacts of projects like this—but we should.
Evidence Based Practice “Best of the Posters” session honoree
Of the 46 projects submitted for consideration at the April 2018 Evidence Based Practice Poster Fair, this project was one of three selected for presentation at the “Best of the Posters Session.” We applaud these efforts to share and spread best practices in delivering high value health care within our community and beyond. Learn more here.
Sharon Ugolini
Utah’s Chief Medical Quality Officer Bob Pendleton describes a strategic challenge faced by many industries, including health care. We are at risk for prioritizing achievement of metrics over our purpose. He challenges us to think beyond metrics to what patients actually need from us: patient-centered, outcome-focused, affordable care.
Sometimes the most impactful change comes from simply asking, “Why are we doing things this way?” Pediatric infectious disease professor Adam Hersh explains the impact of practice inertia on antibiotic treatment in pediatric patients, and how questioning the status quo improved outcomes and reduced cost.
Patients will ask three things of us over the next decade of health care improvement: help me live my best life, make being a patient easier, and make care affordable. To meet those needs health care must shift—from organizing around a patient’s biology to understanding the patient’s biography.