If
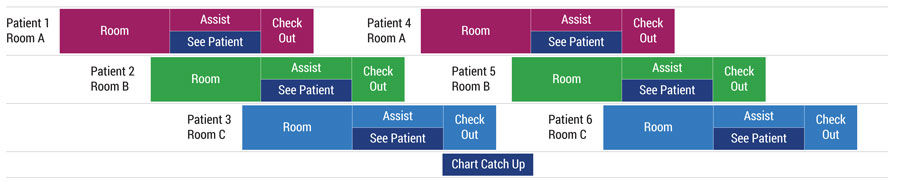
you’ve ever had a suspicious mole removed and declared, “This dermatologist is a rock star,” you were not being quite as hyperbolic it might seem. Value Engineering has been studying and improving clinic flow at University of Utah Health since 2015. When we learned how two dermatologists, Chris Hull and Mark Eliason, run their respective clinics, I thought, that’s how U2 ran their 360 Tour . Their model differs in important ways (and for various reasons) from the flow manager model we’ve introduced to other clinics, but it works well for them.
As of this writing, U2’s 360 Tour (2009-11) holds the record for the highest grossing tour ever, blasting past 2nd place (Rolling Stones’ Bigger Bang Tour, 2005-07) by 32%.
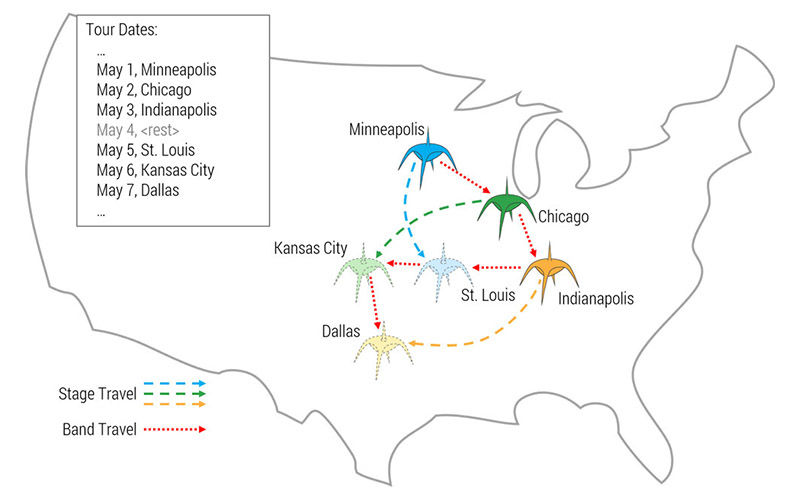
The 360 Tour stage, looking like an aggressive spaceship, was also the biggest ever. If only it could’ve flown intact from city to city. Rather, it was dismantled and loaded into 120 (not a typo) semi-trucks. It took 150 people and four days to re-build it at each new venue. If logistics is your thing you can find out more at the tour’s suitably massive Wikipedia page.