
he COVID-19 pandemic has left clinical workers, from nurses to techs to physicians, exhausted. After years of being overworked and understaffed, even the smallest tasks, like handwashing, can feel impossible.
Nationwide, hospitals and healthcare system are finding that safety and infection control measures are slipping. Recent studies have revealed nurses are missing about half the opportunities for performing hand hygiene. Additionally, the more staff members need to wash their hands, such as in our ICU settings, the less often they are complying with handwashing guidelines.
We’re hearing from staff members that they are too busy to wash their hands or to wait for hand sanitizer to dry before putting on gloves. They have too much going on and begin to wonder: Why waste a minute of my time over and over again to wash my hands or 20 seconds to apply hand sanitizer? Why should I dry out my skin and deal with painful dermatitis?
As a health system, we need to get back to the “why” behind handwashing. We need to look again at why it is so important not only for the health of patients, but for the health of our staff.
We need to remember that our first goal as providers is to do no harm to our patients and that handwashing can prevent harm by preventing infections.
Why is it so hard to do?
The infection prevention team’s hand hygiene barrier survey uncovered perceived and observed many different reasons why handwashing compliance is faltering. The numerous reasons direct care providers don’t wash their hands include but not limited to:
- Hands full of supplies
- Frequent entering and exiting the room
- Poorly located sanitizer or soap dispensers
- Empty or broken sanitizer dispensers
- Automatic sinks and towel dispensers
- Skin dryness and irritation
- Improper glove use
- No handwashing role models
We must address these barriers, which have been identified by staff members, in order to improve handwashing compliance. We have to make it easy to wash hands, and we have to remind ourselves why we do it in the first place.
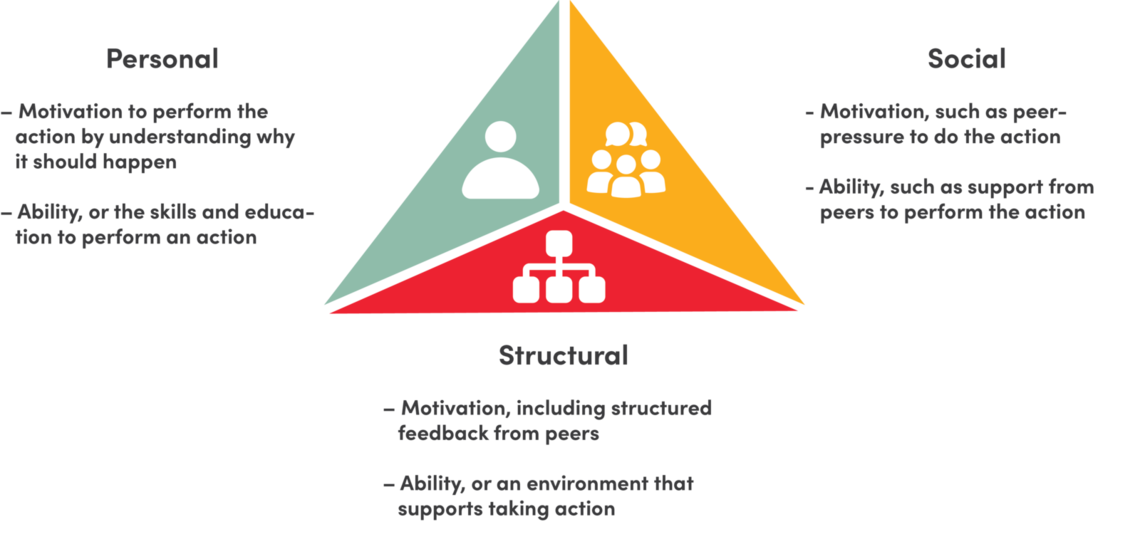
It takes “Six Sources of Influence” to change handwashing behaviors
To really improve handwashing behaviors within our facilities, we can use the influencer model. This model states that there are six sources of influence on our actions and to sustain behavior changes a combination of strategies are needed.
-
Personal motivation to perform the action by understanding why it should happen
-
Personal ability, or the skills and education to perform an action
-
Social motivation, such as peer pressure to do the action
-
Social ability, such as support from peers to perform the action
-
Structural motivation, including structured feedback from peers
-
Structural ability, or an environment that supports taking the action
The influencer model can be used to address any behavior or action. We should use this model to address barriers to handwashing within our patient care units. Each type of influence can reveal strategies we can use, such as:
-
We can improve personal motivation by utilizing vicarious experiences and connecting to moral behaviors and sense of self.
-
We can improve personal ability by reemphasizing the 5 moments and correct techniques for hand hygiene.
-
We can increase social motivation by appointing handwashing champions within each unit who serve as role models who provide positive feedback and just in time coaching/mentoring.
-
We can improve both social ability and structural motivation by setting hand hygiene goals and providing structured feedback linking hand hygiene to patient outcomes.
-
We can create structural ability with clear expectations and ensuring that all dispensers are full, working, and placed properly throughout the facilities.
It all starts at the bedside
All of these efforts begin with leadership from the people who are actually at the bedside, who are experts at the challenges of delivering care. Our team members can be champions in improving handwashing compliance for the whole team. They understand why handwashing does or does not happen.
By re-engaging our teams in this effort, we can improve infection control and safety within our facilities.
Throughout all the interventions ( or actions) to influence behavior changes, we must remember the ultimate reason we wash our hands so frequently when caring for patients is because handwashing stops the spread of infection. It stops us from unintentionally harming our patients. It allows us to protect ourselves, our patients, our family and our friends from illness. Through such a small action, we can have a large impact on lives of others.